SUPPLEMENTARY FILE 4
A re-analysis of the Hall et al. paper “Calorie for Calorie, Dietary Fat Restriction Results in More Body Fat Loss than Carbohydrate Restriction in People with Obesity”
In 2015, Hall
et al. published a highly infuential paper [1] entitled “Calorie for Calorie, Dietary Fat Restriction Results in More Body Fat Loss than Carbohydrate Restriction in People with Obesity” in
Cell Metabolism. The authors restricted dietary carbohydrates
vs. dietary fat for 6 days following a 5 day baseline diet in 19 obese adults confined to a metabolic ward where they exercised daily. Subjects were given both isocaloric diets, the carbohydrate restricted diet (RC) or the fat restricted diet (RF), in random order during each of two stays in a ward. Data seems to suggest that that RF resulted in a greater rate of body fat loss compared to isocaloric RC.
We decided to take a closer look and re-analyze the Hall
et al. data; and we come to the firm conclusion that their conclusion is highly, if not fatally, misleading.
1. Hall et al. data demonstrate that carbohydrate restricted diet (RC) show no risk of body fat accumulation
A widespread postulate, defended by the energy balance theory (EBT), is that during underfeeding body fat loss (FL) is given by the following difference:
Accordingly, RF is expected to result in a greater FL than an isocaloric RC as fat intake is substantially lower. It should be noted, however,
that this is a reasonable hypothesis only if the net fat oxidation is independent of diet macronutrient composition. If the net fat oxidation increases as fat intake increases (and
vice versa), FL can be similar among isocaloric diets that vary greatly in dietary fat content. Hall
et al. data demonstrate that this is indeed the case. Respiratory quotient (RQ) measurements in their
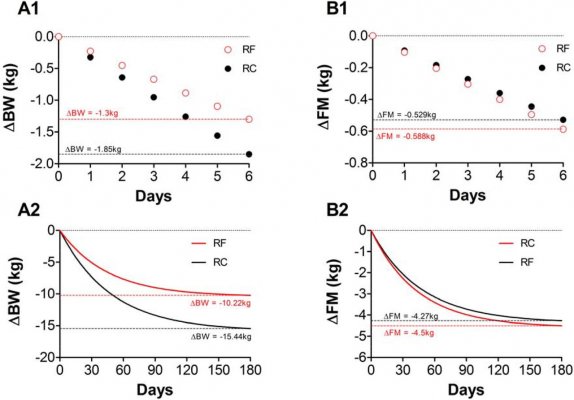
Figure 2C, for example, indicate that fat oxidation increases in proportion to dietary fat intake. Consequently, the characteristic high fat content of RC elicits high levels of fat oxidation, which counterbalances the high fat intake avoiding excessive body fat deposition. This interpretation is valid as dual-energy X-ray absorptiometry (DXA) measurements in Table 3 indicate that fat loss in RC was similar to that of RF even though the latter diet contained substantially less fat (Fat intake: RC = 108g/day vs. RF = 17g/day; Fat loss: RC = –0.529±0.13kg vs. RF = –0.588±0.14kg, p = 0.78). Therefore, it seems that the alleged risk of unwanted fat accumulation with RC diets is highly unlikely and experimentally unjustified.
2. The cumulative fat measurements illustrated in Table 3 (or Figure 3D) are artificial quantities that do not reflect the actual level of body fat loss
DXA measurements in Hall
et al. study are the only direct measurement of fat loss. The presented cumulative fat loss illustrated in Table 3 (or in
Figure 3D) is an undirect estimate of fat loss computed according the following formulas (in grams):
where Daily Fat Oxidation is another estimate calculated by
(see Hall
et al. [1] methods).
In these formulas, the only precise numeric input is “Daily Fat Intake”, whereas the “Daily Net Fat Oxidation” is an
estimate obtained from
estimates which unavoidably increases the measurement inaccuracy. Moreover, if an indirect measurement is indeed accurate, it should be very close to the most precise direct measurements available, such as DXA. Consequently, if cumulative fat loss calculations reported by Hall
et al. are accurate, they should be nearly identical to values measured by DXA, which is clearly NOT the case.
The cumulative fat measurements illustrated in Table 3 (or Figure 3D) are thus artificial quantities that do not reflect the actual level of fat loss.
Nevertheless, Hall
et al. try to convince readers that the direction of accuracy is other way around, i.e., cumulative fat calculations are more accurate than direct DXA fat mass measurements. In the justification of such a proposal, they argue that DXA measurements may be prone to inaccuracies in settings of carbohydrate restriction as this may lead to greater water loss than fat restriction:
“But even high precision methods, such as DXA, may lack the sensitivity to detect small differences in body fat change… Indeed, retrospective analysis [what analysis?] of our data suggests that the minimal detectable difference between the diets for body fat mass using DXA was ⍰0.4 kg. Thus, we suspect that the DXA measurements of fat mass change in the present study were insufficiently sensitive to detect differences between the diets. Furthermore, DXA may provide inaccurate results in situations of dynamic weight change and shifting body fluids… This could be especially important with diets differing in their level of carbohydrate restriction since greater losses of body water are likely with lower levels of dietary carbohydrate.” [1]
It should be noted, however, that DXA fat mass measurements will be mainly unaffected since the amount of water present in the body fat compartment is essentially non-existent. Thus, if any inaccuracy is present, it would be substantially greater for lean mass measurements than for fat mass measurements as total body water is basically localized in the lean mass compartment. This fact, alone, refutes the above mentioned interpretation by Hall
et al.
Sensitivity, nonetheless, is an academic issue with minor relevance in the treatment of obesity. Lets assume, as Hall
et al. claim, that DXA sensitivity is ∼ 0.4kg. This means that if DXA fat mass measurement before a dietary intervention is, let say 35kg, and a particular underfeeding procedure decreases fat mass by exactly 200g (0.2kg) then DXA measurement will still read 35kg as the fat mass change is less than the sensitivity of the instrument. This is, of course, immaterial during typical underfeeding interventions as the fat loss at such procedures substantially exceeds DXA sensitivity.
3. Compared to RF, RC resulted in significantly greater weight loss both experimentally and computationally
Table 3 by Hall
et al. shows that RC resulted in substantially more weight loss than isocaloric RF (RC:– 1.85±0.15kg vs. RF: –1.3±0.16kg, p = 0.022). For instance, the simulation in
Figure 3H shows that, over a six month period, RC leads to about 4kg of extra weight loss compared to RF.


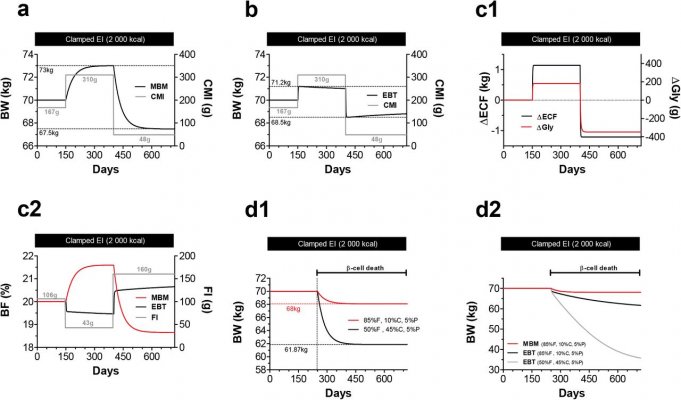
") Olemme MBM-simuloineet myös mm. Hallin tutkimuksen. Hänhän on EBT-leirin "Yli-Jumala". Mikä tässä Hallin ym. metabolisessa kammiossa suoritetussa tutkimuksessa on nyt yhtäkkiä vikana, kun se sopii täydellisesti MBM-pohjaiseen simulaatioon?
Olemme MBM-simuloineet myös mm. Hallin tutkimuksen. Hänhän on EBT-leirin "Yli-Jumala". Mikä tässä Hallin ym. metabolisessa kammiossa suoritetussa tutkimuksessa on nyt yhtäkkiä vikana, kun se sopii täydellisesti MBM-pohjaiseen simulaatioon?