Mitähän helvettiä tossa sitten loppupeleissä oikein lukee?

Ei pahalla mutta nyt meni jäsentely aivan perseelleen.
Ihan hyvä se on. Monesta asiasta erikseen tulee juttua.
Alkuperänen viesti oli, että kasvirasvoihin kannattaa nojata lähtökohtasesti ketodietin. Margariinia ei purematta nielty, jonka ymmärrän ihan täysin varsinkin jos margariini nähdään mitä se oli 40-50 vuotta sitten, eli täynnä transrasvoja. Muutenkaan en näe pointtia miksi pitäisi ottaa perusteluks jos 40-50 vuotta tehdyssä tutkimuksessa olisi ollut vilppiä, kun nämä asiat on vamistettu paljon myöhemmin? Sen aikanen margariini on ollu paskaa!
Sitten vihjaillaan miten hiilihydraateilla parannettava esidiabetes/diabetes on älytöntä; Hiilareita vähentämällä saa hyviä tuloksia, ei tarvitse tosin vetää 20-40grammaan. Ja hiilareiden piikkiin tietenkin menee lisääntynyt diabetes, vaikka sokerin syönti on vähentyny. Tietyissä piireissä. Vaikka kalorien syönti on kasvanut.
Hiilarin korvaaminen tyydyttyneellä rasvalla efekti:
Replacement of carbohydrates with SFA Results from multiple regression analysis (weighted for N) are summarized in Table 3 and demonstrate that for each 1% of dietary energy as carbohydrates replaced with an equivalent amount of SFA, there was a: ▶ significant increase1 in total cholesterol of 0.045 mmol/L (95% CI: 0.03 8, 0.051), in LDL cholesterol of 0.036 mmol/L (95% CI: 0.030, 0.043), in HDL cholesterol of 0.011 mmol/L (95% CI: 0.010, 0.013), in the LDL cholesterol to HDL cholesterol ratio of 0.007 (95% CI: 0.001, 0.014; P = 0.033), in ApoA-I of 8.4 mg/dL (95% CI: 6.4, 10.5) and in ApoB of 3.7 mg/dL (95% CI: 1.7, 5.8); ▶ significant decrease1 in triglyceride of 0.012 mmol/L (95% CI: –0.015, –0.008) and in the triglyceride to HDL cholesterol ratio of 0.016 (95% CI: –0.020, –0.012); and
We performed a meta-analysis of 60 selected trials and calculated the effects of the amount and type of fat on total:HDL cholesterol and on other lipids.
Conclusions: The effects of dietary fats on total:HDL cholesterol may differ markedly from their effects on LDL. The effects of fats on these risk markers should not in themselves be considered to reflect changes in risk but should be confirmed by prospective observational studies or clinical trials. By that standard, risk is reduced most effectively when trans fatty acids and saturated fatty acids are replaced with cis unsaturated fatty acids. The effects of carbohydrates and of lauric acid-rich fats on CAD risk remain uncertain. https://pubmed.ncbi.nlm.nih.gov/12716665/
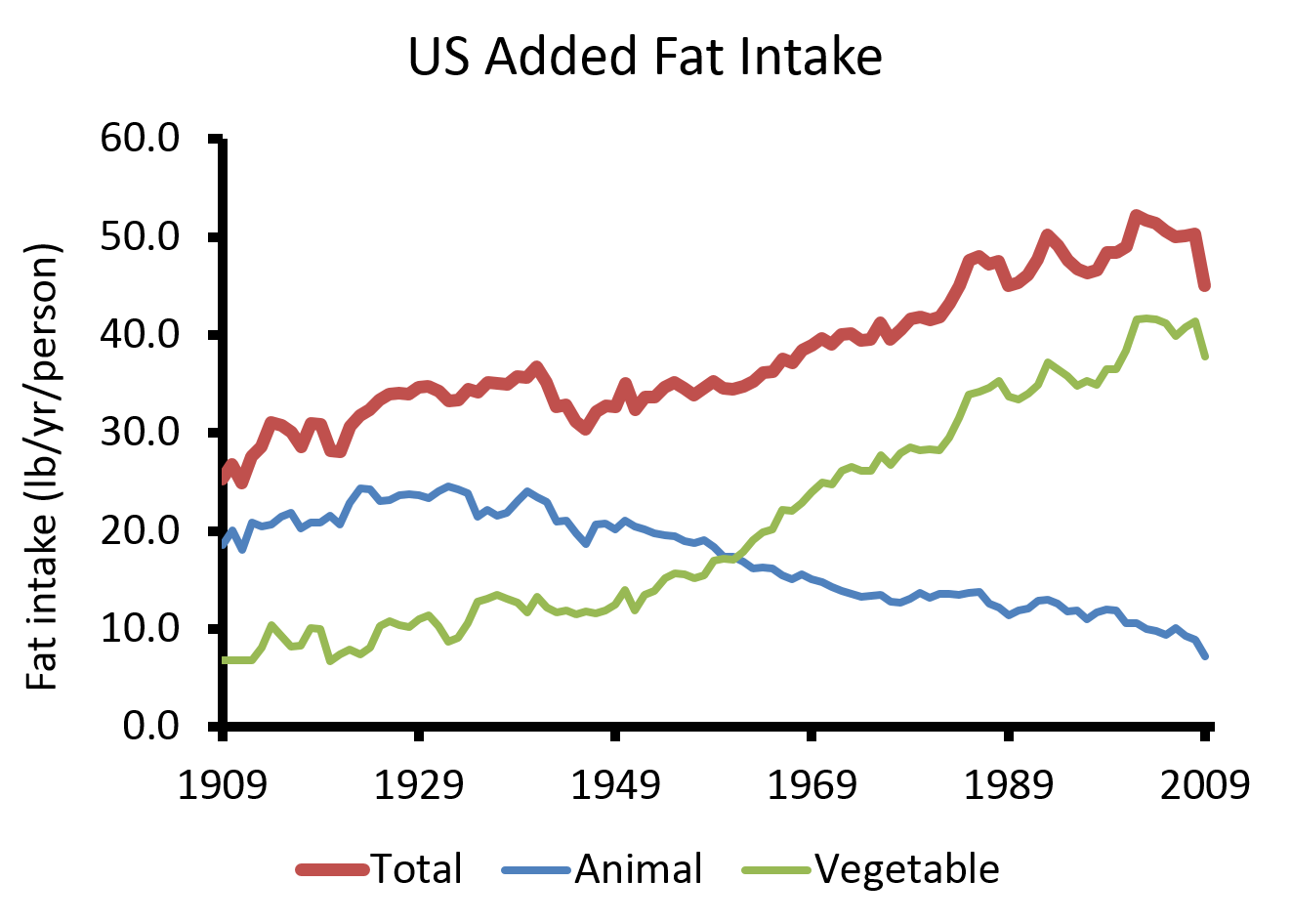
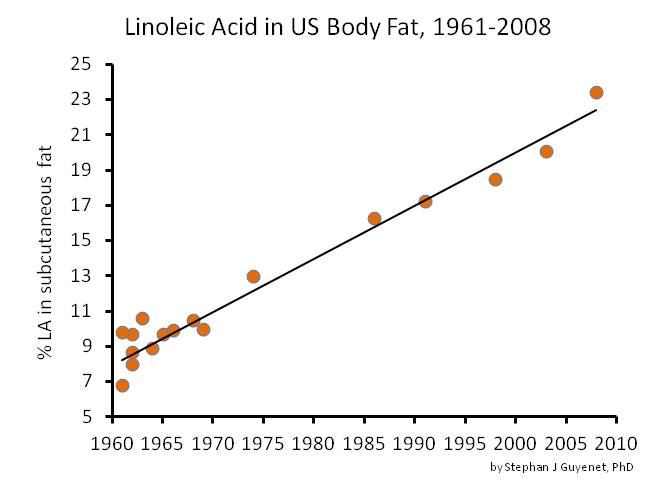
Sitten Minnesota Coronary Experiment-tutkimukseen, sen pääpointti on linoleenihapon(omega6) lisääminen ja tyydyttynyneen rasvan vähentäminen olisi aiheuttanu mm. sydänsairauksien riskin kohoamista. No, paljon myöhemmin tehdyissä tutkimuksissa saturoidun/tyydyttynyt/kovan rasvan korvaaminen kasviöljyillä on hyvä vaihtoehto.
''Kaikessa mediahiljaisuudessa on ilmestynyt Chowdhury’n jälkeen Farvidin ym. etenenvien väestötutkimusten meta-analyysi, jonka mukaan linolihapon runsas saanti ravinnosta suojaa sepelvaltiomotaudilta (16). Tulos havaittiin sekä ns. itsenäisenä tekijänä riippumatta muista tekijöistä, että myös ns. vaihtokauppa-analyysissä tyydyttyneeseen rasvaan kuin myös hiilihydraattiin. Farvidin ja Chowhury’n analyysien keskeisin ero valittuissa tutkimuksissa, analyysit olivat “syöneet sisäänsä” eri tutkimuksia.''
Background: Previous studies on intake of linoleic acid (LA), the predominant n-6 fatty acid, and coronary heart disease (CHD) risk have generated inconsistent results. We performed a systematic review and meta-analysis of prospective cohort studies to summarize the evidence regarding the relation of dietary LA intake and CHD risk. Conclusions: In prospective observational studies, dietary LA intake is inversely associated with CHD risk in a dose-response manner. These data provide support for current recommendations to replace saturated fat with polyunsaturated fat for primary prevention of CHD.
https://pubmed.ncbi.nlm.nih.gov/25161045/
Joten yks tutkimus 40-50 vuotta sitten ei kumoa nykypäivän tutkimuksia. Varsinkin kun osallistujia on 310 000 kun minnesota hommassa oli 9000 eli 34 kertaa suurempi.
We identified 13 published and unpublished cohort studies with a total of 310 602
Prolonged exposure to lower LDL-C beginning early in life is associated with a substantially greater reduction in the risk of CHD than the current practice of lowering LDL-C beginning later in life.

www.ncbi.nlm.nih.gov
In this meta-regression analysis, the use of statin and nonstatin therapies that act via upregulation of LDL receptor expression to reduce LDL-C were associated with similar RRs of major vascular events per change in LDL-C. Lower achieved LDL-C levels were associated with lower rates of major...
pubmed.ncbi.nlm.nih.gov
Abstract
Background: Reduced saturated fat (SFA) consumption is recommended to reduce coronary heart disease (CHD), but there is an absence of strong supporting evidence from randomized controlled trials (RCTs) of clinical CHD events and few guidelines focus on any specific replacement nutrient. Additionally, some public health groups recommend lowering or limiting polyunsaturated fat (PUFA) consumption, a major potential replacement for SFA.
Conclusions: Prolonged exposure to lower LDL-C beginning early in life is associated with a substantially greater reduction in the risk of CHD than the current practice of lowering LDL-C beginning later in life.
The relative risk (RR) of major vascular events (a composite of cardiovascular death, acute MI or other acute coronary syndrome, coronary revascularization, or stroke) associated with the absolute reduction in LDL-C level; 5-year rate of major coronary events (coronary death or MI) associated with achieved LDL-C level.
In this meta-regression analysis, the use of statin and nonstatin therapies that act via upregulation of LDL receptor expression to reduce LDL-C were associated with similar RRs of major vascular events per change in LDL-C. Lower achieved LDL-C levels were associated with lower rates of major coronary events.
Kalorin saanti kasvanu, hiilarin saanti pienentyny, samaten kun diabetes lisääntynyt:
- The number of people with diabetes rose from 108 million in 1980 to 422 million in 2014.
- The global prevalence of diabetes* among adults over 18 years of age rose from 4.7% in 1980 to 8.5% in 2014 (1). https://www.who.int/news-room/fact-sheets/detail/diabetes /https://pubmed.ncbi.nlm.nih.gov/20609967/
Myöskään linolenihappo(omega6) ei ole yhteydessä korkeempaan tulehdukseen vaikka keto piireissä uumoiltu arakidonihappo on se paha:
Results: Decreasing dietary linoleic acid by up to 90% was not significantly correlated with changes in arachidonic acid levels in the phospholipid pool of plasma/serum (p = 0.39). Similarly, when dietary linoleic acid levels were increased up to six fold, no significant correlations with arachidonic acid levels were observed (p = 0.72). However, there was a positive relationship between dietary gamma-linolenic acid and dietary arachidonic acid on changes in arachidonic levels in plasma/serum phospholipids.
Conclusions:
Our results do not support the concept that modifying current intakes of dietary linoleic acid has an effect on changing levels of arachidonic acid in plasma/serum or erythrocytes in adults consuming Western-type diets.
https://pubmed.ncbi.nlm.nih.gov/21663641/
Satunnaistetuissa tutkimuksissa omega-6 rasvahappojen, erityisesti linolihapon, erittäin runsas saanti ei lisää tulehdusta, eikä vähäinen saanti vähennä tulehdusta (
Johnson & Fritsche 2011). Linolihapon saanti ollut tässä systemoidussa katsauksessa mukana olleissa lisäystutkimuksissa noin 2-5-kertainen suomalaiseen saantiin nähden eli 20-50 g/pv vs. 10 g/pv, kun taas vähennystutkimuksissa linolihapon saanti ollut n. 5 g/pv eli puolet siitä mitä keskimääräinen suomalainen saa.
Linolihapon runsas saanti ei ole yhteydessä CRP-tulehdusarvoon väestötutkimuksien meta-analyysissä (
Su 2017)
Tämä selittynee sillä, että minimaalinen määrä vain 0,3-0,6 % linolihaposta ylipäätään muuntuu arakidonihapoksi elimistössä (Demmelmeir 1999) ja sillä, että monissa ruuissa, erityisesti lihassa ja kalassa, on luontaista arakidonihappoa suurempia määriä kuin mitä linolihaposta keskimäärin muuntuu arakidonihapoksi elimistössä. On myös ilmeistä, että arakidonihappopitoisuus on tarkoin säädelty elimistössä.
Ps. Älkää naurako mulle, mulla on herkät tunteet. Nyt on pakko yrittää nukkua, silmät ihan ristissä kun piti käydä kymmeniä tutkimuksia läpi. Toisaalta tää on hyvä, oma osaaminen kasvaa.


")











")